A consultant walks onto a university campus with a mandate to fix the student health access problem. She spends three weeks reviewing utilization data, interviewing the health center director, the VP for Student Affairs, the CFO. She benchmarks against peer institutions. She runs the numbers on every option she knows.
Her recommendation lands in one of three places: hire more staff and expand the clinic, partner with a regional health system, or add a telehealth platform. She presents it with confidence, because those are the options.
And six months later, the wait times are still two weeks out.
Every campus health model in wide use today shares the same structural requirement: the student has to do something before care can happen. Schedule an appointment. Cross campus. Find a private space for a video call. Log into a portal.
At each of those steps, some demand is lost. A student who was going to ask about the anxiety that's been keeping her up decides it's not worth the hassle. A freshman with a sinus infection waits until it's a sinus infection plus a missed exam. A student managing a chronic condition who doesn't have a car and can't get to the off-campus provider just doesn't go.
This isn't a staffing problem. You can't hire your way out of it. The constraint isn't headcount. It's the model itself.
Internal expansion gives universities control and comprehensive care, but it's expensive, slow to scale, and still dependent on students coming to a single facility during business hours. The campus health center built in 1972 has been renovated, but the architecture—show up, schedule, wait—hasn't changed.
Outsourcing to a health system transfers the staffing burden, but usually at the cost of institutional control. And it doesn't change the access equation. The clinic is still in one place. The appointment is still required.
Telehealth extended the reach of mental health care and created real after-hours access—those are genuine wins. But behavioral health represents the majority of telehealth utilization for a reason: telehealth cannot conduct a physical exam, take a blood pressure reading, or use a stethoscope. The 40 to 50 percent of freshmen who don't have a car can technically access a telehealth visit—but only if they can find somewhere private on a campus designed to be social. Most of them don't bother.
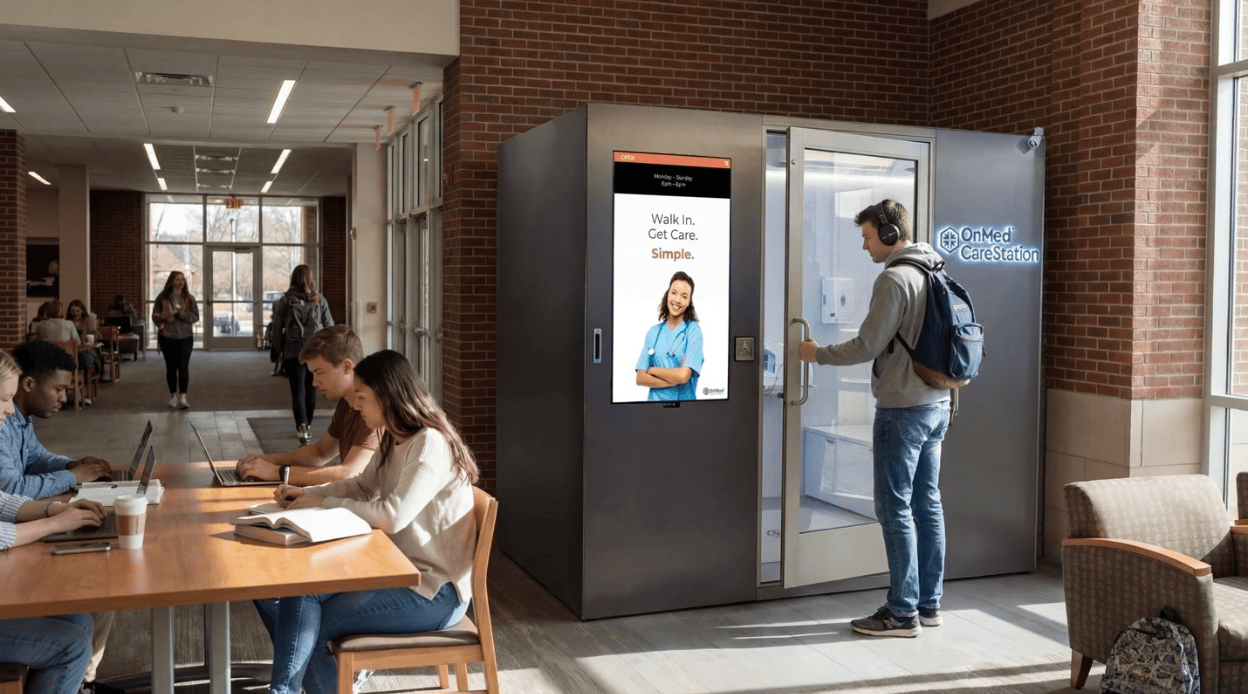
Distributed on-campus care infrastructure places care directly into the residential hubs, dining halls, and student unions where students already spend their time. No appointment, no crossing campus, no scheduling portal, and no waiting room. Walk in, get care, walk out—in about 20 minutes.
The impact shows up in the data. In deployed distributed care models, 92% of visits are resolved on-site without escalation to a specialist, urgent care, or ER. Forty percent of users become repeat patients—a number worth sitting with in a population where getting a student to seek care at all is the primary challenge. Campus health centers that add distributed care see a 33% reduction in overflow burden and a 25% reduction in operational costs. Not because students stopped needing care. Because the care got to them before the problem got bigger.
The model also changes the mental health equation. When care is private, stigma-free, and available in the same place a student goes for a sinus infection, students who would never walk into a counseling center start getting screened. The barrier isn't willingness. It's visibility. Remove the visible act of seeking help, and utilization goes up.
Seventy percent of students factor healthcare access into their college choice. Fifty-four percent of students who leave name health as a contributing reason. At a private university, one retained student represents $135,000 in protected four-year tuition. A 1% retention improvement at a 5,000-student institution is $6.75 million.
The OnMed CareStation™ isn't a replacement for your health center—it's the piece that makes everything else work better. It absorbs the high-frequency, episodic demand that floods the clinic at midterms and finals, freeing clinical staff for the complex cases that actually require them. It deploys in 45 days, requires no construction or additional hiring, and costs less than one-tenth of one percent of average annual tuition.
The access gap on your campus is structural. Incremental investment in models that share the same structural flaw produces incremental results. The institutions that close the gap will be the ones that change the architecture.
Explore how the OnMed CareStation™ delivers distributed, on-campus care infrastructure—and compare all four models in the Campus Health Operating Model Evaluation Framework.
Follow along as we continue to redefine the healthcare landscape and bring the OnMed CareStation to communities across the U.S.