The American healthcare system is exceptionally good at treating complexity. What it struggles with is far simpler: a starting line.
Most Americans enter the system in one of three ways. They make an appointment with a primary care physician and wait weeks or months—if one is even available and taking new patients. We’re in the middle of a primary care shortage. They show up at an urgent care center and hope for the best. Or they go to the emergency room for something that was never an emergency. None of these is a true starting point. All three are somewhere in the middle of a journey that never had a beginning.
That absence has a name. It’s called the first mile problem, and it shapes everything that follows.
More than 100 million Americans don’t have regular access to primary care—a number that has nearly doubled since 2014, according to KFF Health News. The consequences of the primary care shortage ripple outward in ways both human and financial.
Without a consistent first stop, patients make decisions in the dark. They wait too long. They go to the wrong place. They arrive somewhere expensive and overloaded, presenting with something that was manageable three weeks earlier.
The emergency department has quietly become that first stop for millions. Avoidable and non-emergent ER visits are costing the system an estimated $168 billion annually in misdirected care. The average cost of treating a primary-care-treatable condition in the ED is $2,032. The same visit at a physician’s office runs $167. That is a 12-times cost gap, paid over and over, by a system with no front door.
For the patient, the cost of no starting point isn’t just measured in dollars. It’s a second copay for a visit that should have been the first. It’s a referral to a specialist with a three-month wait, a redundant test, a bill that arrives before a diagnosis does. Every misdirected step adds expense, delay, and risk—and none of it would have happened with the right first stop.
The problem isn’t just cost. It’s trajectory. Research consistently shows that care delayed is condition worsened. A missed diagnosis today is a hospitalization tomorrow. A patient who can’t reach a first stop doesn’t just not get better—they get more expensive to treat.
According to KFF, an estimated 167 million Americans—across every age group—delay or forgo needed care each year, with 120 million doing so specifically because of inadequate access to primary care. That delay doesn’t disappear. It defers. And deferred care compounds.
The most important thing a first point of care does is not treat. It’s decide.
A true first mile healthcare model doesn’t attempt to be everything. It does two things with precision: it resolves what can be resolved right now, and it routes everything else to exactly the right place. That’s triage in its truest form—not a hospital concept, but a care-delivery philosophy. See clearly. Act when appropriate. Move intelligently when not.
When triage works, the entire downstream system works better. The specialist receives a patient who has already been assessed. The imaging center isn’t processing a referral that should never have been made. The ER is treating emergencies. The primary care physician has capacity for the patients who actually need continuity. Every node in the network functions closer to its design.
When triage is absent, care becomes reactive, fragmented, and expensive. The patient who can’t find a starting point becomes a diagnostic odyssey. Each encounter rebuilds context from scratch. Each provider sees a partial picture. The system doesn’t fail at the point of treatment—it fails at the point of entry.
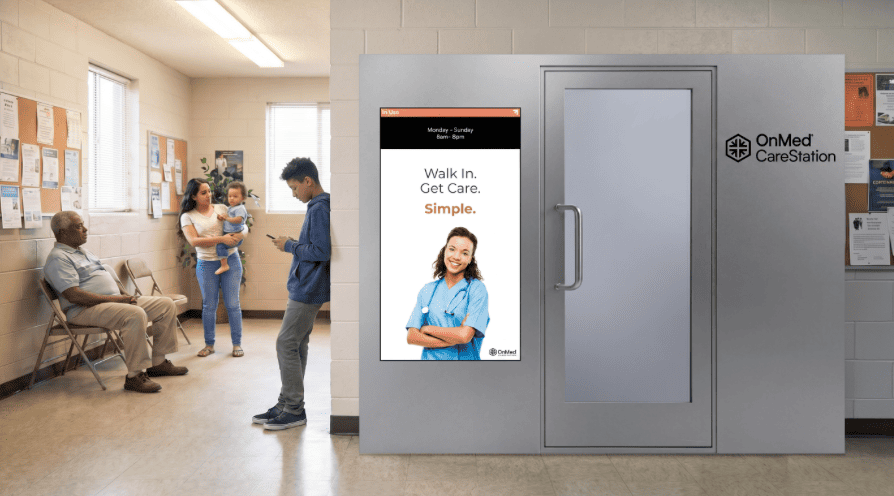
The OnMed CareStation™ is a purpose-built first mile healthcare infrastructure. It can be deployed anywhere there is an electrical outlet—in communities that have no primary care physician, in workplaces where the nearest urgent care is miles away, in campuses and retail environments and health system campuses where care access today is a waiting room or a search result.
Inside the CareStation, a licensed clinician, on a 55” screen, conducts a full clinical-grade evaluation using integrated diagnostic tools including digital stethoscope, HD cameras, blood pressure monitoring, pulse oximetry, thermal imaging, and otoscope. The patient gets a real assessment, not a symptom check. And critically, they get a decision: treated now, or routed to exactly the right next step.
That second path matters as much as the first. 86% of CareStation patients are fully diagnosed on-site without escalation. That means 86% of visits resolve at the starting point. The other 14% leave with a clear, informed referral rather than a guess. Either way, the patient exits with clarity—not a prescription to figure it out later.
The results speak to what happens when people have access to a real first stop. 78% of CareStation users report they have no primary care physician—which means that for most of the people seen, the CareStation is not supplementing their care. It is their care. And 58% of visits divert from an emergency room or urgent care setting, shifting the cost of that encounter from a $2,032 ED visit to an appropriate primary care interaction.
A well-designed first mile doesn’t just benefit the individual patient. It recalibrates the economics of every system it connects to.
For employers, the math is direct with this on-site healthcare solution. Healthcare costs are projected to exceed $18,500 per employee in 2026, according to Mercer. A meaningful portion of that cost lives in avoidable ER utilization, untreated chronic conditions, and absenteeism that traces back to a care gap. When employees have immediate access to a first mile care point, issues resolve before they compound. The $2,032 ER visit becomes a fraction of that. The missed diagnosis becomes a caught one.
For health systems, the CareStation creates network alignment. Patients who would otherwise be lost in the system—no PCP, no care continuity, no relationship with a provider—become reachable. The CareStation identifies them, assesses them, and routes them into the right care pathway. That’s patient acquisition, population health management, and ER diversion happening simultaneously at the same point of entry.
For payers, it’s an intervention at the moment of highest leverage. Care that is appropriately triaged and delivered at the first mile is categorically less expensive than care that is deferred, misdirected, or escalated unnecessarily. The first mile is where cost is shaped, not just incurred.

Healthcare often measures success at the end of the journey: was the surgery successful, was the condition managed, was the patient discharged. The first mile changes the frame.
When a patient walks into the CareStation, they leave with one of two things: care delivered, or a clear and appropriate next step. No ambiguity. No “we’ll need to refer you” without context. No “go to the ER if it gets worse” from someone who hasn’t examined them. The starting point is defined, and the path forward is specific.
That clarity compounds. A patient who knows where they stand makes better decisions. A care team that receives a triaged patient moves faster. A system where every entry point is intelligent and intentional is a system that performs.
The first mile isn’t a convenience. It’s the foundation. Interested in learning how OnMed can help close your healthcare access gap? Contact Us.
More than 100 million Americans lack regular access to primary care—a number that has nearly doubled since 2014. The shortage is not a single-cause problem. It is structural: fewer physicians entering primary care relative to demand, an aging population generating higher utilization, and geographic maldistribution that concentrates providers in urban centers while rural and underserved communities go without.
First mile healthcare refers to the initial point of entry into the care system—the starting line that most Americans currently lack. A true first mile care model does two things with precision: it resolves what can be resolved immediately, and it routes everything else to exactly the right next step.
→ Read more: Healthcare Access in America | Beyond Telehealth: Why Diagnostic Tools Unlock Real Care
Employer healthcare costs are projected to exceed $18,500 per employee in 2026. A meaningful portion of that cost lives in avoidable ER utilization, untreated chronic conditions that escalate before they are caught, and absenteeism that traces directly back to a care access gap. When employees have immediate access to a first mile care point—at or near their workplace—issues resolve before they compound. The $2,032 ED visit becomes a fraction of that cost. The missed diagnosis becomes a caught one. For self-insured employers, 58% ER diversion from a CareStation deployment is a direct and measurable claims reduction. For fully insured employers, it improves utilization patterns and renewal positioning.
→ Read more: The Greatest Untapped Source of ROI — Employee Health | The Hidden Cost Centers Employers Aren't Measuring
The CareStation functions as a first mile access point that intercepts care before it reaches the emergency department. 58% of CareStation visits divert from an ED or urgent care setting, shifting the cost of that encounter from a $2,032 emergency visit to an appropriate primary care interaction. 86% of patients are fully diagnosed and treated on-site without specialist escalation, meaning the vast majority of visits resolve at the starting point rather than cascading into downstream referrals.
→ Read more: Returning Emergency Departments to Emergency Medicine | How Health Systems Are Reducing ED Strain, Cutting Leakage, and Expanding Access Without Building
Follow along as we continue to redefine the healthcare landscape and bring the OnMed CareStation to communities across the U.S.

.jpg)
